
Dissemination and implementation (D&I) science/research is the scientific method to promote the spread and the systematic translation of evidence-based interventions, including practices and policies, into routine practice.1,2 Dissemination and implementation research and practice is integrated within the broader and more established concept of translational research. The rapidly evolving field of D&I research aims to accelerate the slow and often inequitable translation of evidence-based interventions into real-world settings.1 Despite its importance, D&I research continue to be sparse across sports and exercise medicine fields as researchers continue to mainly conduct clinical and traditional discovery research rather than hybrid or full D&I research.2 For example, a recent systematic review examining best practices for disseminating and implementing neuromuscular training warm-up exercises showed that core D&I hybrid studies, i.e., type 2 and type 3 hybrid effectiveness-implementation randomized controlled trials (RCTs), remain very limited (n = 2, 2.9%) and pure D&I RCTs were nonexistent.3 It is, however, promising that 19 (32%) studies used D&I theories/frameworks/models.3 Beyond exercise-based interventions, the knowledge translation gap affects several interventions and cuts across health disciplines,1 including sports and exercise medicine and related fields.2 More D&I studies are needed to bridge this gap. In this editorial, we discuss the need to ask D&I-focused translational research questions and provide directions on hybrid research approaches.
WE NEED TO ASK THE RIGHT QUESTIONS FOR REAL-WORLD IMPACT TO HAPPEN
“Does the intervention work?” This is the research question we have been asking for several years. We need to start shifting away from questions like “Does exercise (in whatever form e.g., for fall prevention, sports injury prevention, management of osteoarthritis, or tendinopathy) work?” We know that many exercise interventions are clinically efficacious/effective, as demonstrated by numerous research works, cumulating in systematic reviews, overview of reviews, and expert consensus/clinical guidelines.4–6 However, most of these interventions have been examined without considerations for D&I, hence without D&I outcomes evaluated. We need to pivot to questions like: “What D&I strategies support the rapid translation and sustainment of interventions in local clinical and community settings?” “Are these interventions effective in real-world settings, especially when tailored to local contexts?” “What are the determinants of implementation for the intervention” and “How do we help patients/clients/athletes adhere to the intervention?”
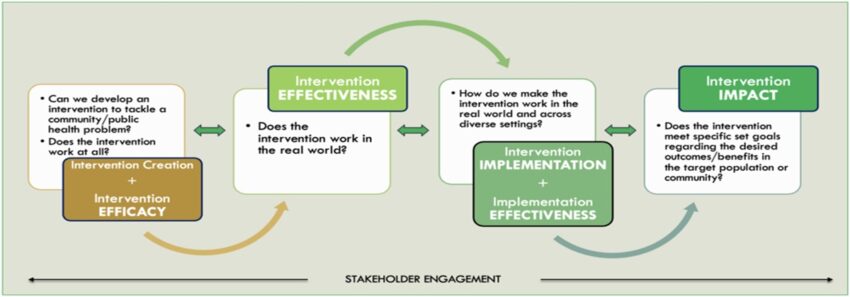
The Essential Translational Research Questions and Pathway to Intervention Impact provides a framework to generate and prioritize research questions that will drive clinical interventions toward impact (Figure 1). Indeed, not all researchers need to focus on D&I studies, but all researchers can play some role in the translational research spectrum.7 Interconnecting clinical and D&I research with essential translational research questions is important for a rapid and impactful knowledge translation. Researchers should continue to efficiently engage relevant stakeholders in shaping research questions and design throughout the translational research continuum while applying relevant D&I research principles.8 Depending on the research question of interest and the current state of evidence for an intervention, research studies may be completely clinical (as many interventional studies are currently), hybrid (eg, the RCT by Peterson et al9), or completely D&I (eg, this quasi-experimental study by Owoeye et al.10).
Essential Translational Research Questions and Pathway to Intervention Impact. Interconnecting clinical and D&I research with impact-driven translational research questions is important for rapid knowledge translation. This pathway is often bidirectional as the development of effective clinical interventions and implementation strategies are dynamic and continually adapted to diverse contexts and refined over time.
HYBRID STUDIES ACROSS MULTIPLE RESEARCH DESIGNS
Hybrid studies blend components of clinical effectiveness and D&I research within the translational research continuum. The concept of hybrid studies was originally initiated for RCTs in the form of effectiveness-implementation studies and has been used in clinical and public health research.11 However, new knowledge necessitates that hybrid research methods and measures are integrated into observational research (referred to as observational-implementation studies) and potentially other designs, and across multidisciplinary biomedical research fields.12
Any study with research questions related to both clinical and D&I research is a hybrid study, and they should be described as one. To foster a common language consistent with the D&I field and advance D&I science in sports and exercise medicine, studies with elements of D&I science, no matter how little, should indicate the degree to which D&I is a focus using the effectiveness-implementation (a hybrid classification system for RCTs, quasi-experiments based on their extent of D&I focus) or observational-implementation approach (a hybrid classification system for observational studies based on their extent of D&I focus), depending on the study design. Studies combining elements of clinical and D&I research should be expressly identified as a type 1, 2, or 3 hybrid study. Hybrid typologies are mainly determined by study outcome(s); however, exposure(s)/effect modifier(s) may have a clinical or D&I orientation, depending on the research question.
Table 1 describes hybrid research types with sample study purpose and relevant study outcomes. In a hybrid type 1 study, clinical outcomes (eg, injuries, pain) are prioritized (about 80%), and there is a minimal focus (about 20%) on D&I outcomes.2,11 Although the exposures considered in type 1 studies are usually clinically oriented (eg, an RCT evaluating the effectiveness of the 11+ structured warm-up exercises, a neuromuscular dynamic warm-up program for preventing sports injuries,13 vs traditional warm-up on injury outcomes), there could be situations where researchers are interested in exposures that are contextualized in D&I (eg, a modified 7-minute 11+ aimed at addressing the implementation barrier of limited time vs the traditional 15-minute 11+ program on injury outcomes), to see if the modified 11+ (in this case, an implementation strategy in the form of intervention adaptation) losses or maintains its initial injury prevention efficacy. In type 1 studies, D&I outcomes may be limited to implementation barriers and facilitators in a secondary or tertiary study aim.
Hybrid Research Types
| Hybrid Type | Examples of Research Aims* | Study Examples | Primary Outcome is Clinical |
Primary Outcome is D&I |
Secondary Outcome is Clinical |
Secondary Outcome is D&I |
| 1 | (1) Evaluate the clinical effectiveness of an intervention (primary) and explore implementation determinants, including barriers and facilitators (secondary) (2) Evaluate the effectiveness of D&I strategies (primary) with or without an exploration of implementation determinants, including barriers and facilitators (secondary) |
Digital interventions to promote physical activity among inactive adults: A study protocol for a hybrid type I effectiveness-implementation randomized controlled trial13 | ✓ | ✓ | ||
| 2 | Evaluate the clinical effectiveness of an intervention and the effectiveness of D&I strategies (about equal focus) | Brief physical activity counselling by physiotherapists (BEHAVIOUR): Protocol for an effectiveness-implementation hybrid type II cluster randomized controlled trial14 | ✓ | ✓ | ||
| 3 | Evaluate the effectiveness of D&I strategies (primary) and explore the clinical effectiveness (e.g., using nonexperimental designs) of an intervention subjected to a substantial amount of adaptation during implementation (secondary) | Evaluation of an injury prevention program (prep-to-play) in women and girls playing Australian football: Design of a pragmatic, type III, hybrid implementation-effectiveness, stepped-wedge, cluster randomized controlled trial9 | ✓ | ✓ |
*As applicable in effectiveness-implementation studies.
A type 2 hybrid study has about equal balance of clinical and D&I outcomes in combination with appropriate study aims.2,11 A key requirement for type 2 hybrid studies is that researchers need to be clear about the intervention (ie, clinical intervention) components versus D&I strategy components and how each is tested.2,11 In a type 3 hybrid study, the focus is mainly (about 80%) on D&I outcomes (eg, self-efficacy, fidelity, adaptation vs clinical outcomes).2,11 The hybrid typing system is currently mostly used in effectiveness-implementation studies employing experimental (RCTs) and quasi-experimental designs. Direction on how to apply the typing system in observational-implementation studies is in development but yet to be clarified in the D&I literature.12 A broad terminology of hybrid observational-implementation study may be adopted by researchers at this time. This will help implementation support specialists, practitioners, and researchers easily identify observational studies that are relevant to knowledge translation.
CONCLUSIONS AND FUTURE DIRECTIONS
Sports and exercise medicine researchers are encouraged to ask translational research questions that integrate hybrid research approaches, that is, combining clinical and D&I objectives and outcomes in their work, using relevant research designs and methods, including qualitative and mixed methods. Depending on the stage where an intervention is in the translational research spectrum, and using appropriate implementation theories, models, and/or frameworks, researchers should consider incorporating and evaluating relevant D&I research objectives across a broad range, including the evaluation of (1) intervention effectiveness; (2) intervention adherence or nonadherence; (3) implementation readiness; (4) contextual barriers across implementation actors; (4) the determinants of implementation; (5) sustainability of evidence-based interventions in clinical practice and public health; (6) the effectiveness and cost-effectiveness of theory-informed D&I strategies for evidence-based interventions; and (7) the adaptation of evidence-based interventions within local contexts.
References